


How Can We Fix The Broken Insulin & Diabetes Medication System?
An exploration.

Hello, friends!
In our last post, we talked about how Ranked Choice Voting could, if implemented more widely, make our Democracy better. Today, we’re going to talk about one improvement that a better electoral system could lead to for the average person. I’d like to focus on a conversation I overheard today (Friday), and its implications, but the long-and-short is:
Medication to treat Diabetes (such as Insulin) needs to be free.
Let’s talk, because there’s a lot to talk about.
Diabetes Medication Is Too Expensive, But How Much Is It?
The conversation centered around two people who, if my proximity-based eavesdropping was accurate, are both well-experienced with the disease. One had it, and one had a loved one who did. Both were clear-cut: Diabetes medication costs an astronomical amount, and it shouldn’t. After all, access to insulin is a life-or-death matter for diabetics. No insulin? No living.
Finding useful data on a static cost per unit of insulin, is no easy task. That’s because of two factors: First, the American healthcare system, in its Byzantine madness, charges different consumers different amounts based on what (if any) insurance they have; second, that there are a lot of different brands of insulin, all of which cost different amounts.
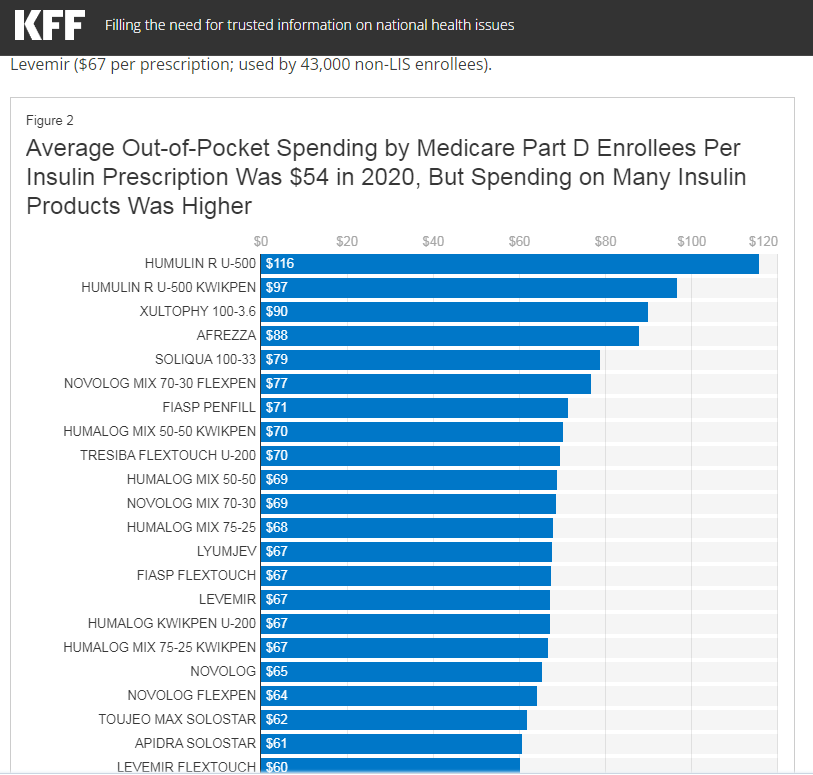
The Kaiser Family Foundation (KFF), which is thankfully not linked to the Kaiser Permanente healthcare system, reports that in 2020 the average cost of an Insulin prescription for a Medicare Part D patient was approximately $54. That sounds fairly reasonable, assuming you need one prescription for a month; a “mere” $648/year cost of not dying. Of course, Medicare requires you to be 65 years old to sign up, and that doesn’t apply to all versions of insulin, just some, but, it’s a starting number.
NBC News reports that Dr. Adam Gaffney, a physician based out of Massachuchets, more recently quoted a monthly price over over $1,000 for those who have no insurance. That’s, what, a meager $12,000/year for the privilege of being alive! And, who knows, the version of insulin you need to live might be even more!
If that sounds morally bankrupt to you, that’s because it is.
That’s why companies like Eli Lilly flipped out when a fake Twitter account pretending to be the pharmaceutical giant announced that they would give their insulin products away for free: It put a clear target on their business practices. According to NPR, insulin prices have skyrocketed 600% in the past twenty years! While that surely leads to bumper-crop profits, it also leads to people who can’t afford what they need deciding to “ration” what little they have, often fatally.
Digging A Bit Deeper Into Insulin Cost Drivers.
I’m going to quote KFF one more time and cite one of the charts they used. I’m doing this to give you, dear reader, some idea of just how many different types of insulin exist.
Now, let’s back up over a century.
Insulin was first identified by name in May of 1922 - or, put another way, over a hundred years ago, now. In January of 1923, a patent was issued to some of the scientists who worked on the project, which they sold to the University of Toronto for a grand, whopping total of $1. Yes, there are no zeros after that number. One dollar.
The idea was that insulin ‘belonged to the world.’ Today, sure enough, much of the rest of the world has plenty of access to it! World Population Review, a website dedicated to collecting data, indirectly (rather nebulously) cites a 2018 RAND Corporation study (potentially this ASPE-affiliated data, released in September of 2020?) which chronicled the cost of insulin across the ten most expensive countries for it in the world, and the results are not very surprising:

Insulin is cheaper in every other country in the world - by a tremendous margin - than it is in the United States. Part of the reason for that is changing: Up until the passage of the Inflation Reduction Act, Medicare could not negotiate drug prices with manufacturers. Now, at least, Medicare will have that power - though that does not necessarily imply lower prices for privately insured, or uninsured people.
One aspect of the problem comes down to something a little out of my depth - different forms of insulin. According to the American Diabetes Association, there are five different types of insulin. Mostly, the factor is whether the insulin is quick-acting or long-lasting. Different types, and sub-types, will cost different amounts. Part of that makes sense as a matter of manufacture: Some kinds might just be harder to produce than others!
Part of it comes down to a phenomenon called “evergreening,” where tiny changes made to medicines enable producers to renew their patents - and thus exclusivity - on the production of that medication. In the US, pharmaceutical companies get a period of time where they are the only ones allowed to produce and distribute the medications they invent. This is done to promote innovation (“You made this great thing, you get a temporary monopoly as payback”), but this already-questionable system is frequently abused. Mylan Pharmaceuticals did something like this with the EpiPen.
Finally, at least for the purposes of this discussion, part of it comes down to the barriers of entry for new competitors to enter the market in the first place. Investopedia has a list of these prohibitions that could serve well for the sake of this conversation. One of them is getting FDA approval - a necessary evil, to make sure snake oil isn’t billed as miracle cures. Another of them is, surprise, patent litigation! If you want to make your own insulin company, you have to worry about lawsuits (justified or not) by other producers. That means, hypothetically, that California’s effort to produce its own might well be challenged in court. There’s also the cost of actually getting the equipment - and scientific know-how - to make it. Granted, it appears this can be done literally in your own garage, but making production function at a significant scale requires significant investitures into equipment - all to create a product which may be threatened by lawsuits a-plenty.
While this is surely an imperfect encapsulation of the costs of insulin manufacture, it should provide enough food for your imagination to comb the depths.
Solutions To The Insulin Crisis
We already mentioned that California is taking a national lead in this regard, establishing its own manufacture facilities. Other states (I’m looking at you, New York) could follow suit, which would theoretically increase supply and thus lower prices.
We also touched on the fact that the recent Eli Lilly scandal might ‘encourage’ them to lower prices of their own accord - a face-saving move, to be sure, but a beneficial move nonetheless.
Perhaps most importantly - for older Americans - is that the Inflation Reduction Act actually sets a maximum price ceiling of $35 for insulin under Medicare. This, combined with Medicare’s new ability to negotiate prices with manufacturers, means that the costs for insulin and other Diabetes medications might be lower for Medicare patients.
Of course, corporations might just off-load those costs onto the uninsured and privately-insured, in order to protect their record-pace profits, but that’s another story.
Last, but far from least, there’s a little solution called “Medicare For All,” which would be a total overhaul of how the nation handles healthcare through the conception of a single-payer system. That would solve the cost problem for everyone.
And, yes, we will touch on Medicare For All further in a lovely little spiral whenever we discuss medical affairs on The Progressive Cafe.
Next up: Talking about Chronic Pain.
Thank you for reading The Progressive Cafe. If this article has helped you, please consider signing up for our mailing list. This article is by Jesse Pohlman, a sci-fi/fantasy author from Long Island, New York, whose website you can check out here.